Researchers at Johns Hopkins School of Medicine’s Center for Psychedelic and Consciousness Research have submitted a pre-print research paper titled: Serotonergic antidepressant use is associated with weaker psilocybin effects (Gukasyan et al., 2022). A preprint is a publicly-available full draft of a research paper that is pending peer review.
The current dogma is that serotonergic antidepressants reduce the psychedelic effects of psilocybin by blocking its mechanism of action (partial agonism of the 5HT2a receptor). However, this dogma is fairly unsubstantiated as of yet by science. The only clinical trial to date on SSRI + psilocybin was done just earlier this year and carried one big limitation. Becket et al. conducted a randomized controlled study on a small sample of participants who were administered escitalopram over 14 days then dosed once with synthetic psilocybin; they found no significant effect on the mystical qualities of the psychedelic experience. However, the average time of onset of an SSRI to treat depression is about 2 weeks, and its maximum effect can take upwards to 6 weeks, or even more, so we still do not know how ongoing SSRI use would effect a psilocybin experience in the real world.
Gukasyan et al. tries to answer the question: 1) how is a psilocybin experience affected by common antidepressants? 2) how is a psilocybin experience affected by recently coming off antidepressants? They ran a survey study to answer these questions. Responses were collected between Sept 2020 and Nov 2021 via online advertising. Participants were asked if they had taken psilocybin 1) before being on an antidepressant 2) while taking an antidepressant or 3) after stopping an antidepressant. Those who answered yes to Q2 and Q3 proceeded to further data gathering. Some of the Qs they asked respondants included:
- number of experiences
- type of antidepressant used
- psilocybin dose
- subjective effects after taking psilocybin
- presence/absence of an antidepressant holiday before taking psilocybin
- presence/absence of adverse effects
- presence/absence of serotonin syndrome
- how long ago they stopped their antidepressant (if relevant)
- other medications they take
- other substances they took at the time.
Of the 2,625 participants who completed the survey and reported taking psilocybin during or after an antidepressant, their reports were filtered further to ensure their validity for the study. The sample was 91% white, 55% male, 54% at least had a Bachelor’s degree, and most were located in the USA. Researchers wanted only participants that could report on their psilocybin experiences before and after being on an antidepressant while on the same dose and type of fungal psilocybin, or compare their experience to that of friends who took the same dose but aren’t on antidepressants. With these criteria, among other criteria that ensured the reports were sensibly coherent and comprehensive, they arrived at 596 reports of taking psilocybin with an SSRI, SNRI, or bupropion, that were from 455 survey respondents.
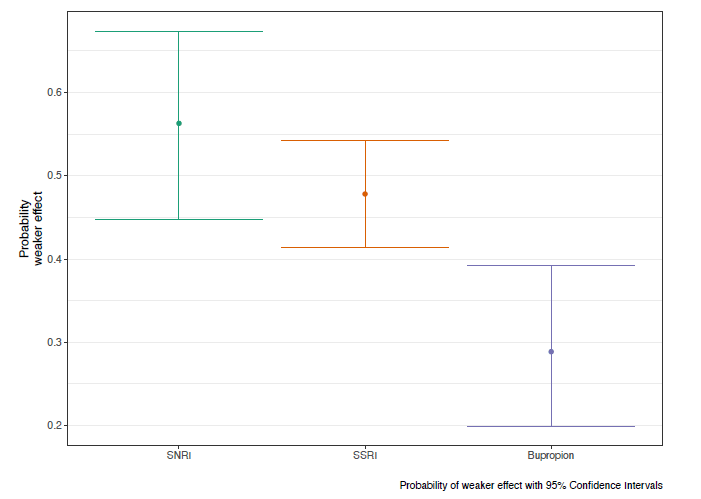
Their results were reported as the adjusted probability of weaker than expected effects of psilocybin when co-ingested with an SNRI, SSRI, or bupropion. The probability of weaker effects was 0.59 for SNRIs, 0.48 for SSRIs, and 0.2 for bupropion. This means: SNRIs were the most likely to blunt psilocybin’s effects and bupropion was the least likely.
Now let’s break down these results further:
- 57.2% used another substance during the experience, most commonly cannabis or alcohol
- The most common antidepressants reports were escitalopram (n=146) and sertraline (n=124)
- Antidepressant doses were not included as they did not significantly affect data outcomes and were fairly variable
- Of those who reported reduced psilocybin effects, 51.7% attempted to overcome this with a higher dose of psilocybin
- There was no significant effect on psilocybin experience from taking an antidepressant holiday
- 5.7% of respondents believes they had an adverse effects from combining psilocybin with an antidepressant
- Only 8 respondents (0.7%) believed they experienced serotonin syndrome as a consequence of combining psilocybin with an antidepressant
So what’s the big picture? Although survey data is of lower scientific rigor, this large scale study did an excellent job of limiting confounding variables and collecting only high quality online reports of outcomes on combining psilocybin + common antidepressants. Safety outcomes are very favorable and serotonin syndrome risk is negligible. Outcomes are as we would expect: SSRIs, SNRIs, and bupropion blunt psilocybin’s effects with bupropion’s effect being the least. Given the role of expectancy bias in psychedelic outcomes, I wonder if bupropion’s blunting effects are a magnification of true pharmacologic blunting of psilocybin since bupropion has negligible effect on the serotonin receptor system. Keep in mind that about half of respondents showed any blunting! This would suggest not everyone on an antidepressant will have their psilocybin experience blunted. I am excited to see clinical trial outcomes on drug-drug interactions with psychiatric medications so we can see the role of medication dosing and the inclusion of other combinations with psilocybin such as mirtazapine and aripiprazole.
Stay tuned for PART 2 where we discuss these provocative outcomes:
“This dampening effect on psilocybin effects may last as long as 3 months following antidepressant discontinuation”
